All information is based on current medical research (2020-2026). Written specifically for patient education by Dr. Antonio Gargiulo. This article does not replace a consultation with your gynecologist or healthcare provider.
This article is the companion to “What Is Adenomyosis and Could I Have It?” If you have not read that piece yet, we recommend starting there.
Introduction: Two Names, One Complicated Picture
Adenomyosis and endometriosis are two of the most confused gynecological conditions. They share a name root, similar hormonal drivers, overlapping symptoms, and a frustrating tendency to be missed or misdiagnosed for years. They also frequently occur in the same patient at the same time. Yet they are not the same disease – and understanding the difference, the overlap, and the gap in how medicine handles them can make a real difference in the care you receive.
Sisters, Not Twins – What Makes Them Different
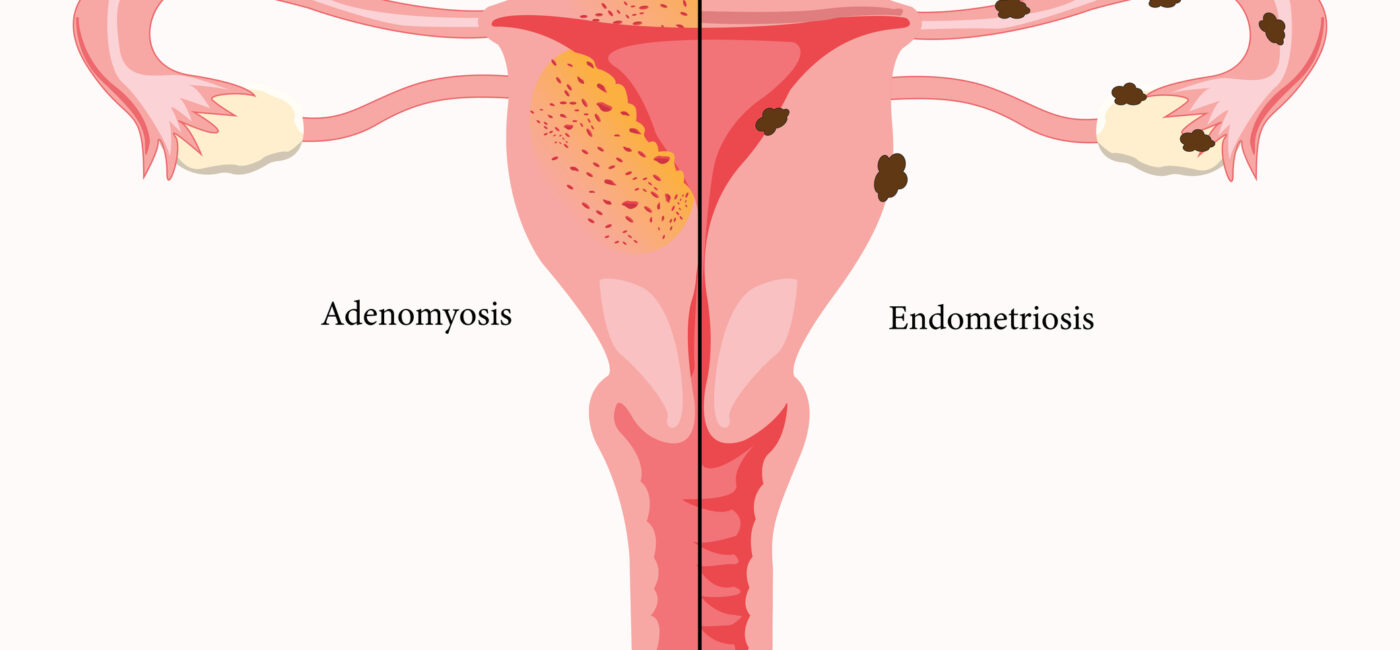
Both conditions involve endometrial-like tissue growing where it does not belong. The location is what separates them:
– In adenomyosis, the tissue grows inside the muscle wall of the uterus.
– In endometriosis, similar tissue grows outside the uterus – on the ovaries, fallopian tubes, bladder, bowel, or other pelvic and extra-pelvic structures.
Think of it this way: adenomyosis is an “inside job” and endometriosis is an “outside job.”
Both are fueled by estrogen. Both cause inflammation. Both can be painful. But they behave differently, affect different structures, and produce different dominant symptoms:
| Feature | Adenomyosis | Endometriosis |
| Location of tissue | Inside the uterine muscle | Outside the uterus |
| Most common symptom | Heavy menstrual bleeding | Severe pelvic pain |
| Typical age of diagnosis | 35-50 years | 25-35 years |
| Effect on fertility | Yes — can impair implantation | Yes — can block tubes and damage ovaries |
| Responds to estrogen | Yes | Yes |
| Frequently co-occurs with the other | Yes | Yes |
A large 2026 study found that heavy menstrual bleeding was the dominant feature of adenomyosis (present in 64% of patients), while more severe pain characterized endometriosis. Women who had both conditions together had the highest overall burden – more bleeding, more pain, and lower quality of life than those with either condition alone.
How Often Do Adenomyosis and Endometriosis Occur Together?
Very often. Studies consistently show that a large proportion of women who have one condition also have the other. They share similar hormonal drivers, similar inflammatory processes, and some overlapping genetic patterns. When endometriosis is found at surgery, adenomyosis is frequently present but goes undetected – precisely because laparoscopy cannot see inside the uterine wall (see our companion article for more on this).
This coexistence matters clinically. A woman whose endometriosis is treated surgically but whose adenomyosis goes unrecognized may continue to have significant symptoms — especially heavy bleeding and pelvic pressure – that may not respond to endometriosis treatment, because they are being caused by a different disease entirely.
Are Adenomyosis and Endometriosis the Same Disease?
This is one of the most actively debated questions in gynecology. Some researchers argue that adenomyosis and endometriosis are two distinct phenotypes – i.e. different expressions – of the same underlying disease of the uterus and its lining. Others maintain they are separate conditions that share biological mechanisms but have different origins and different natural histories.
The current weight of evidence suggests they are closely related but distinct entities. They can occur independently, they respond somewhat differently to treatment, and they have different dominant symptoms. But the biological kinship is real and has practical implications: a patient with one condition should always be evaluated for the other.
A Critical Gap –Adenomyosis Has No Validated Staging System
One of the most important differences between these two conditions is not biological – it is organizational. And it has direct consequences for how well your disease can be described, tracked, and treated.
Endometriosis has been classified and staged for decades. The most widely used system is the revised American Society for Reproductive Medicine (rASRM) classification, which stages the disease from I (minimal) to IV (severe) based on the location, depth, and extent of lesions and pelvic adhesions. The AAGL and the ENZIAN classifications, developed more recently, offers a more detailed surgical map of the disease. These systems give doctors a shared language: when one specialist describes a patient as having “stage III endometriosis with deep infiltrating lesions,” another specialist anywhere in the world understands exactly what that means.
Adenomyosis has no equivalent. Several classification proposals have been published – mostly based on MRI or ultrasound features such as the location, size, and pattern (focal vs. diffuse) of the disease – but a 2022 review of the literature concluded that none of these proposals has been validated and that there is currently no widely accepted and validated system for adenomyosis. A few pilot scoring systems are being tested in small studies, but none has achieved international consensus.
It is worth noting honestly that even endometriosis classification systems have been criticized: a 2021 systematic review found that most show “no or very little correlation with patient outcomes” such as pain or quality of life. So, the contrast is real but not absolute – endometriosis is ahead in having attempted and partially validated systems, while adenomyosis is still at the starting line.
Why does this matter for you?
Without a shared staging system, two women both diagnosed with “adenomyosis” may have vastly different disease burdens – yet their diagnoses look identical on paper. It becomes difficult to compare studies, choose treatments based on disease extent, or predict how your symptoms might evolve. Establishing a validated classification system for adenomyosis is one of the most pressing unmet needs in this field – and one that the medical community is actively working to address. Meanwhile, your doctor is going to be in charge of understanding and explaining the extent of your specific adenomyosis picture and the specific impact it can have on your general and reproductive health: this is a very sophisticated level of counseling that only a few professionals (namely, reproductive endocrinology subspecialists with a special interest in the endometriosis spectrum) have the real expertise to provide.
What This Means for Your Quality of Life
Adenomyosis is often called “benign” in medical textbooks. Technically true – it does not cause cancer or spread to other organs. But it can have a profound impact on everyday life. Women with adenomyosis frequently report:
– Missing work or school during heavy, painful periods
– Avoiding social activities due to unpredictable bleeding
– Strain on intimate relationships because of painful sex
– Anxiety and depression related to chronic pain and fertility concerns
– Anemia and fatigue from blood loss
Studies using validated quality-of-life questionnaires consistently show that adenomyosis significantly reduces physical functioning, emotional well-being, and sexual quality of life. Women with diffuse (widespread) adenomyosis report worse outcomes than those with focal (limited) disease. When adenomyosis coexists with endometriosis, the combined symptom burden is even greater.
The word “benign” should never be used to minimize what you are experiencing. You deserve to have your symptoms taken seriously, fully evaluated, and treated — not just for one condition, but for the complete picture of what is happening in your body.
How to Advocate for Yourself
Given how often these conditions are missed, misdiagnosed, or diagnosed one at a time, here is what the evidence supports:
a) If you have been diagnosed with endometriosis, ask whether adenomyosis has been specifically evaluated with a transvaginal ultrasound or MRI focused on the uterine wall.
b) If you have heavy bleeding alongside pelvic pain, do not assume it is all endometriosis. Heavy bleeding is a hallmark of adenomyosis – NOT endometriosis – and may require different treatment.
c) If you had a “normal” laparoscopy but still have heavy bleeding and pelvic pressure, adenomyosis may be the undiagnosed cause. A laparoscopy can NEVER rule it out.
d) Seek care from a specialist who has experience with both conditions and who is committed to using imaging routinely as part of the evaluation – not only as a preoperative tool. Our practice has made this commitment decades ago, and partners with only the best imaging experts in the field.
Read first: “What Is Adenomyosis and Could I Have It?” for a full explanation of the disease, its causes, and how it is properly diagnosed.
Sources We Used
So You Can Read Them, Question Them, and Decide for Yourself
We believe that informed patients are empowered patients. In an age where artificial intelligence and open-access science place original research within reach of anyone, you have every right to go to the source, read it yourself, and form your own conclusions. Patient education on this website is taken seriously: we do not simplify at the cost of truth, and we do not ask you to take our word for it.
Every statement in this article carries two layers of accountability. It has been filtered through the critical eye of Dr. Antonio Gargiulo, drawing on four decades of clinical and surgical experience in reproductive medicine and advanced gynecologic surgery. And it is independently traceable to a peer-reviewed scientific publication, listed below with its full reference and digital identifier (DOI), so you can retrieve and read the original source at any time.
We see healthcare as a shared responsibility between doctors and patients. Shared responsibility requires shared access to information. These references are not a formality. They are here for you.
1. Gallone A, Santalucia M, Giani M, et al. **Adenomyosis and Endometriosis: a differential diagnosis by clinical symptoms.** *Journal of Endometriosis and Uterine Disorders.* 2026. DOI: 10.1016/j.jeud.2026.100153
2. Donnez J, Stratopoulou CA, Dolmans M-M. **Endometriosis and adenomyosis: Similarities and differences.** *Best Practice and Research: Clinical Obstetrics and Gynaecology.* 2023. DOI: 10.1016/j.bpobgyn.2023.102432
3. Maruyama S, Imanaka S, Nagayasu M, et al. **Relationship between adenomyosis and endometriosis; Different phenotypes of a single disease?** *European Journal of Obstetrics, Gynecology, and Reproductive Biology.* 2020. DOI: 10.1016/j.ejogrb.2020.08.019
4. Kyllo H, Mangham C, Whitmore G, et al. **Preoperative factors associated with the diagnosis of adenomyosis and coexistent endometriosis at hysterectomy.** *American Journal of Obstetrics and Gynecology.* 2024. DOI: 10.1016/j.ajog.2024.02.131
5. Tellum T, Munro M. **Classifications of Adenomyosis and Correlation of Phenotypes in Imaging and Histopathology to Clinical Outcomes: a Review.** *Current Obstetrics and Gynecology Reports.* 2022. DOI: 10.1007/s13669-021-00320-5
6. Kobayashi H, Matsubara S. **A Classification Proposal for Adenomyosis Based on Magnetic Resonance Imaging.** *Gynecologic and Obstetric Investigation.* 2020. DOI: 10.1159/000505690
7. Sinha S, Agarwal M, Bhadani P, et al. **Development and validation of sonological classification and scoring system for uterine adenomyosis: A pilot study.** *F1000Research.* 2022. DOI: 10.12688/f1000research.125700.2
8. Keckstein J, Saridogan E, Ulrich U, et al. **The #Enzian classification: A comprehensive non-invasive and surgical description system for endometriosis.** *Acta Obstetricia et Gynecologica Scandinavica.* 2021. DOI: 10.1111/aogs.14099
9. Hudelist G, Valentin L, Saridogan E, et al. **What to choose and why to use — a critical review on the clinical relevance of rASRM, EFI and Enzian classifications of endometriosis.** *Facts, Views and Vision in ObGyn.* 2021. DOI: 10.52054/FVVO.13.4.041
10. Vermeulen N, Abrao M, Einarsson J, et al. **Endometriosis classification, staging and reporting systems: a review on the road to a universally accepted endometriosis classification.** *Human Reproduction Open.* 2021. DOI: 10.1093/hropen/hoab025
11. Abrao MS, Andres MP, Miller CE, et al. AAGL 2021 Endometriosis Classification: An Anatomy-based Surgical Complexity Score. Journal of Minimally Invasive Gynecology. 2021;28(11):1941-1950.e1. DOI: 10.1016/j.jmig.2021.09.709
12. Mak J, Leonardi M, Espada M, et al. External Validation of the 2021 AAGL Endometriosis Classification: A Retrospective Cohort Study. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2025. DOI: 10.1016/j.ejogrb.2025.02.018
13. Loring M, Chen T, Isaacson K. **A Systematic Review of Adenomyosis: It Is Time to Reassess What We Thought We Knew about the Disease.** *Journal of Minimally Invasive Gynecology.* 2020. DOI: 10.1016/j.jmig.2020.10.012
14. Gorpenko AA, Chuprynin V, Smolnova TY, Buralkina N. **Clinical-anamnestic features and life quality of patients with nodular and diffuse adenomyosis.** *Medical Council.* 2021. DOI: 10.21518/2079-701x-2021-13-68-76
15. Chapron C, Vannuccini S, Santulli P, et al. **Diagnosing adenomyosis: an integrated clinical and imaging approach.** *Human Reproduction Update.* 2020. DOI: 10.1093/humupd/dmz049
16. Yang J, Li X, Peng Y, et al. **Pathogenesis of Adenomyosis: An Integrated Review of Cellular Origins, Molecular Mechanisms, and Intersecting Diseases.** *Journal of Cellular and Molecular Medicine.* 2026. DOI: 10.1111/jcmm.71129